|
 Most people need to use corrective lenses
to improve their eyesight at some point in
their lives. Myopic people usually start
early, as do people with astigmatic
vision. People who are far-sighted can
manage until they get older, when their
eyesight deteriorates and they need
glasses for reading.
Most people need to use corrective lenses
to improve their eyesight at some point in
their lives. Myopic people usually start
early, as do people with astigmatic
vision. People who are far-sighted can
manage until they get older, when their
eyesight deteriorates and they need
glasses for reading.
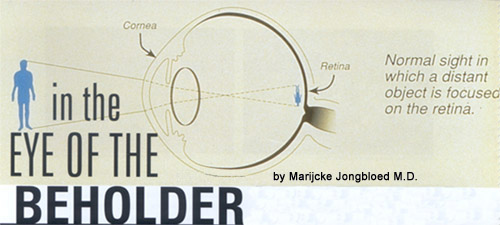
Less
than perfect vision is caused by a change
in the focal length of the optic system
that is the eye. If the focal length is
too long it needs to be reduced in order
for the image to be seen sharply; if it is
too short, it needs to be lengthened.
Spectacles have been used for ages (the
Chinese invented them) and besides being
useful, they have evolved into fashion
accessories. But there are disadvantages
to having to wear glasses. In sports they
can be hazardous, in jungles or the Dubai
summer they fog up. And along with car
keys, they always are misplaced! They are
expensive and scratching or breaking
easily damages the lenses.
The advent of the contact lenses in the
50s addressed some of the
inconveniences of glasses. The apparent
invisibility of contacts was great for
people who were self-conscious about
wearing glasses. They also could engage in
activities that were previously
prohibitive with glasses such as
athletics and physically active careers.
Especially when the long-wear lenses came
onto the market, people happily exchanged
their specs for these flimsy bits of
transparent material. Still, even lenses
get lost Infections of the eye are
sometimes caused and certainly exacerbated
by the wearing of lenses.
It was only a matter of time until someone
came up with the idea that the correction
needed to improve vision could be applied
to the eye itself. Before the appearance
of computers and laser beams, the main
tools available to an ophthalmologist were
a scalpel, a steady hand, a medical
background and perhaps some engineering
knowledge. The premise was that they could
modify the shape of cornea, and then
possibly they could effect permanent
improvement to their patients vision.
(The cornea is the clear dome on the front
of the eye; it is in reality a lens, which
provides about 80% of the focus power of
the eye). The first procedure to show the
possibility of achieving a positive result
was called radial keratotomy or RK.
This is method, in which the qualified eye
surgeon would make series of cuts (usually
4 to 8) in the cornea with a scalpel, in a
pattern that resembles a spoke wheel.
These cuts are fairly deep, more than 90%
of the thickness of the cornea. Later on
lasers have been used to make these cuts,
but with little improvement on the result.
Unfortunately there were many limitations
and complications - some of them resulting
in permanent blindness. It was not
something that I ever recommended as
elective surgery.
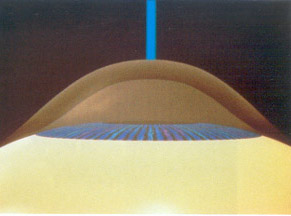
In the last decade new technology has
brought better solutions for poor vision. Photorefractive
keratectomy (PRK)
is a procedure, in which the cornea is
re-shaped to provide the correction that
the eye needs for sharp vision. It sculpts
the focussing power of correcting glasses
or lenses directly into the cornea. This
is done with lasers, which produce an
intense beam of energy with a very precise
wavelength. Lasers were first used
in 1960 and have undergone many
technological changes since that time,
becoming ever more precise and controlled.
The excimer laser can be precise to 0.25
nm, which is one quarter of a micron. The
surgery needed for myopia consists of
removing tissue from the centre of the
cornea, while the correction for
hypermetropia occurs in the periphery,
leaving the central cornea untouched.
Astigmatism can also be corrected by
removing extra tissue in a specific axis
of the eye.
In the early days there were a few
drawbacks to having PRK done. There used
to be quite a bit of postoperative pain
and there were also problems with haze
afterwards. Recuperation took several days
to weeks. Recently there has been progress
in treatment of these two problems, so
that the procedure is now virtually
painless and haze is rarely encountered.
The recuperation time is now considered to
be around two to five days.
A new method was developed that is called LASIK
or "Laser assisted in situ keratomileusis"
(sometimes also referred to as ALK-E). In
LASIK surgery the cornea is cut from the
side to form a lid that remains hinged at
one end.
The sculpting of the cornea is
carried out below this lid, which is then
closed over the area and grows back on.
The advantage of this procedure is that
fewer nerve endings are cut so that the
post-operative pain is reduced. There is
very little trouble with haze and glare
and the recuperation period is measured in
hours and days rather than weeks.
 The disadvantage of the LASIK surgery is
that in order to cut the lid, the pressure
of the eye has to be raised more than 60
mmHg (while the normal pressure is less
than 20 mmHg) in order to be able to make
a clean and smooth cut into the cornea.
This is done by applying a suction cup
around the top of the eye. Even though the
pressure is only raised for a few minutes,
it can already do harm in eyes that are
specifically sensitive to raised pressure.
Another risk is in the cutting of the lid
itself. If the cut is made too shallow the
lid will have a hole in it and if it is
cut too deep the eye may be perforated. In
the postoperative phase, the flap may
become unhinged and can be lost or it
heals off-centre, creating vision
disturbances. The debris created by the
cutting and abrading process can
accumulate along the edge of the flap
creating a sand-ripple effect, known as
the "Sands of the Sahara" effect
- again a visual disturbance that is
unpleasant. There is more chance of an
infection festering underneath the lid and
scarring is also a possibility.
The disadvantage of the LASIK surgery is
that in order to cut the lid, the pressure
of the eye has to be raised more than 60
mmHg (while the normal pressure is less
than 20 mmHg) in order to be able to make
a clean and smooth cut into the cornea.
This is done by applying a suction cup
around the top of the eye. Even though the
pressure is only raised for a few minutes,
it can already do harm in eyes that are
specifically sensitive to raised pressure.
Another risk is in the cutting of the lid
itself. If the cut is made too shallow the
lid will have a hole in it and if it is
cut too deep the eye may be perforated. In
the postoperative phase, the flap may
become unhinged and can be lost or it
heals off-centre, creating vision
disturbances. The debris created by the
cutting and abrading process can
accumulate along the edge of the flap
creating a sand-ripple effect, known as
the "Sands of the Sahara" effect
- again a visual disturbance that is
unpleasant. There is more chance of an
infection festering underneath the lid and
scarring is also a possibility.
Photorefractive Keratectomy (PRK)
has been done in Dubai for almost ten
years by Dr. Niaz Ahmed Khan,
Consultant Ophthalmologist at the Al Zahra
Medical Centre on Sheikh Zayed Road, who
is one of the leading Eye specialists in
the Middle East. Dr. Khan did his medical
studies in Pakistan and his specialty
post-graduate education in London, UK.
Having more than 30 years of experience,
Dr. Khan was the pioneer in introducing
the RK and PRK to the Middle
East. I have started with RK
back in 1987, says Dr. Khan. This
procedure was only OK for patients, who
had to correct low grade of Myopia, maybe
up to 3.0 or 3.5, but could not
address the problems of hyperopia
(farsightedness) at all. Due to the deep
incisions in the cornea, there were a lot
of postoperative complications, but thank
God, we didnt loose any eye.
In 1993 Dr. Khan was the first Eye
Specialist to introduce the PRK to
the Middle East. He has by now treated
more than 1600 patients in UAE with PRK
and more than 5000 case from abroad and
has not had any serious complications. He
estimates that the risk of the only
complication (haze) is less than 1 %.
The PRK is a procedure that
takes only about a minute on each eye,
continues Dr. Khan. The technology now
days is so advanced and the laser is so
precise, that the postoperative
complications that can occur a very minor
and very rear (under-correction or
over-correction) and can easily be
treated.. I also should stress, that
besides cleaning the eye (after inserting
unaesthetic drops) the surgeon is not
touching the eye at all, the whole
procedure is done by the laser beam and is
totally painless.
The prognosis of a person with
Myopia of up to 6.0 to have a 20/20
vision after the surgery are very good.
For higher dioptries sometimes a second
minor correction is needed
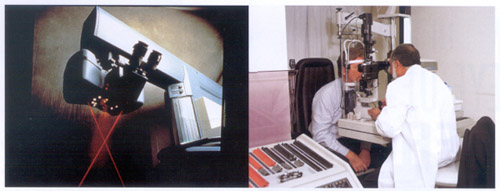
 A consultation for refractive eye surgery
starts with a medical history and a
general eye exam, at which time the exact
level of loss of vision is assessed. The
eye pressure is measured and the eye is
examined minutely for any sign of
superficial or deep infection or
abnormality. Then a special examination is
done in which the topography of the cornea
is recorded on a chart; this is done by
computer. Every irregularity of the
surface of the eye, specifically of the
central part that is the cornea, is
represented on a colourful map showing
"ups" and "downs" just
as in a topographical map of a landscape.
A consultation for refractive eye surgery
starts with a medical history and a
general eye exam, at which time the exact
level of loss of vision is assessed. The
eye pressure is measured and the eye is
examined minutely for any sign of
superficial or deep infection or
abnormality. Then a special examination is
done in which the topography of the cornea
is recorded on a chart; this is done by
computer. Every irregularity of the
surface of the eye, specifically of the
central part that is the cornea, is
represented on a colourful map showing
"ups" and "downs" just
as in a topographical map of a landscape.
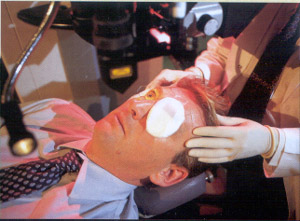
For the actual procedure, the data are fed
into a computer, which directs the laser
beam. The patient lies back on a chair
looking up into a beam of green light that
shines down into his eye. The eye is
anaesthetized with eye drops and the
eyelids are fixed in a clamp to prevent
blinking. The laser beam is centered on
the exact spot of the cornea by two
separate beams of red light that have to
meet the green beam at the exact level of
the cornea. Then the laser beam is used to
take away the precise amount of tissue
from the exact locations determined
beforehand in the topographical exam. The
procedure takes only a few minutes. Both
eyes are usually done in the same session.
The abraded area is covered with a clear
contact lens, which covers the nerve
endings that have been cut in the
procedure and therefore reduces
post-operative pain.
Afterwards the patient is given
painkillers, antibiotic and
anti-inflammatory eye drops and checked
again after a few days, at which time the
contact lens is removed.
Most people are back into their
normal routine within a week. The visual
acuity is immediate.
In eyes that need corrections of more than
6 or 7 dioptries some haze can develop,
which is treated with steroid drops for
three months. Dr. Khan has
treated eyes with Myopia of
- 0.75 as well as - 25(!) and
hypermetropic eyes from +1 to +8. Now
Astigmatism is easily corrected too.
So now can we all have lives without
spectacles? Alas, that is not the case.
Some people with myopia can read without
glasses even in old age. After PRK
treatment they would be able to spot
eagles in the sky without glasses, but
they would need reading glasses for the
newspaper.
There is a solution even for this:
mono-vision treatment, in which only one
eye is corrected by surgery and the other
not. That enables a person to see into the
distance with the operated eye and read
without glasses with the untreated eye. It
does reduce depth vision, for which you
need both eyes. Several of dr. Khan's
patients have had this done and are happy
with it.
At the end of the day, this is elective
surgery, which means it is not necessary
to save a person's life or cure a nasty
disease. However, it can do a lot to
improve the quality of life and it is
great that people nowadays have the choice
to do the surgery or continue to live with
their (minor) handicap.
|